What causes swallowing difficulties? Can acid reflux cause dysphagia?
Dysphagia occurs when the normal function of the oesophagus is impaired. The oesophagus is a hollow muscular tube with valves at its top between the throat or pharynx (upper oesophageal sphincter, UOS) and bottom between the stomach (lower oesophageal sphincter, LOS). Its sole function is to take food from the mouth into the stomach. Its muscles and valves are coordinated by nervous reflexes.
Swallowing can be impaired by disorders affecting the throat such as following a stroke. However, oesophageal disorders causing oesophageal dysphagia do so by either compression of structures outside the oesophagus or pathology within its wall either affecting the nerves, muscles or lining (mucosa). Occasionally a foreign body may impact within the hollow tube itself (lumen) but almost always because of an underlying condition affecting the oesophagus.
Problems causing dysphagia outside the oesophagus include;
- Thyoid gland enlargement (goitre)
- Malignancy of organs adjacent to the oesophagus in the neck, chest and abdomen
- Blood vessels (known as dysphagia lusoria)
- Lymph nodes
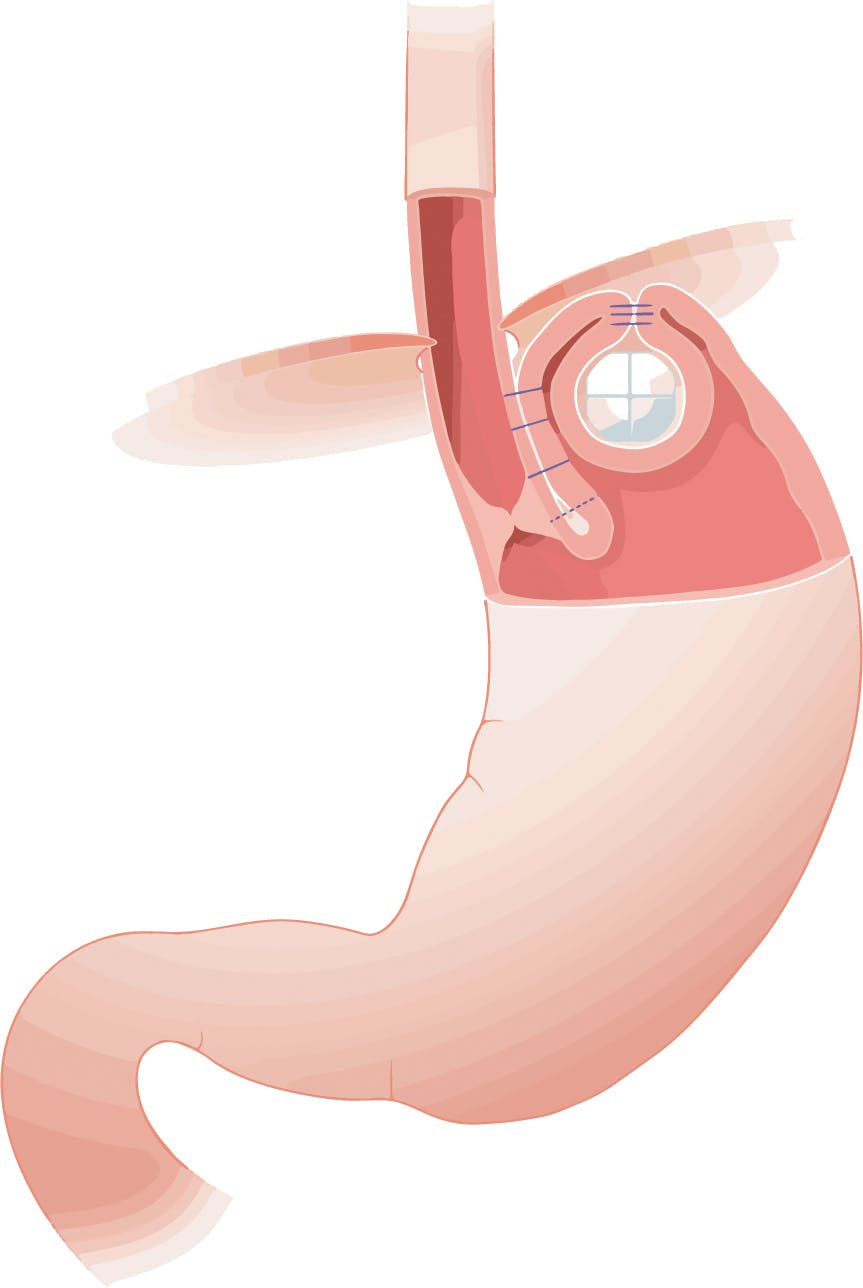
- Following surgery such as fundoplication
- Large hiatus hernias
Problems causing dysphagia within the oesophageal wall include;
- Inflammation including reflux oesophagitis, Eosinophilic oesophagitis, fungal infections, Crohn’s disease
- Benign narrowing (strictures) including reflux associated (peptic) strictures, following radiotherapy, scleroderma and webs
- Malignant narrowing including adenocarcinoma and squamous carcinoma
- Problems affecting the nerves and muscles. The process of action in the nerves and muscles is known as “motility” and diseases causing disordered motility include achalasia (a primary motility disorder), Raynaud’s and reflux associated “ineffective oesophageal motility” (a secondary motility disorder)
How is dysphagia diagnosed?
A diagnosis should always be sought in patients presenting with dysphagia. Malignancy and structural causes should be ruled out. Disorders of oesophageal function can be assessed with x-rays and physiology testing.
Tests for dysphagia include;
- Gastroscopy: Otherwise known as upper GI endoscopy this involves inserting an endoscope through the mouth or nose into the oesophagus and then through the stomach and duodenum (together known as the “foregut”). The endoscope has a high definition camera enabling the operator to look for structural abnormalities such as hiatus hernias. They will also evaluate the lining of the foregut, for instance identifying oesophagitis, benign and malignant narrowing (strictures). If necessary samples of tissue (biopsies) can be taken for analysis. The examination can be performed with local anaesthetic spray, intra-venous sedation or under general anaesthetic.
- Laryngoscopy. These are techniques duing which a clinician, usually an ENT surgeon will examine the throat.
- Indirect laryngoscopy:
This uses a small mirror held at the back of your throat. The examining specialist will shine a light on the mirror to view the throat area.
- Fiberoptic laryngoscopy (nasolaryngoscopy):
This test employs a small flexible telescope. This is passed through your nose and into your throat after a local anaesthetic spray is used to numb the throat. This is the most common way that the voice box is examined. This procedure typically takes less than 1 minute.~
- Direct laryngoscopy:
This employs a tube called a laryngoscope. This procedure allows the doctor to see deeper in the throat and to remove a foreign object or sample tissue for a biopsy. It is performed under general anaesthetic. - Contrast swallow. Patients swallow a liquid, usually Barium and multiple x-rays are then performed. This allows a radiologist to identify structural abnormalities such as narrowing (strictures) or hiatus hernias as well as functional abnormalities such as evidence of reflux.
- High Resolution Oesophageal Manometry (HRM). Manometry allows objective evaluation of oesophageal motility and the swallowing mechanism. A small flexible tube called a catheter is passed through the nostril and down into the oesophagus. The tube has tiny sensors along its length which measure the pressure exerted by the muscles and valves in the wall of the oesophagus. The patient will then be asked to demonstrate swallowing liquids and solids according to a specific protocol whilst the catheter relays the information to a computer which can also generate images based upon the recorded data. HRM is able to diagnose specific abnormalities associated with swallowing problems such as Achalasia, Diffuse oesophageal spasm and ineffective motility associated with GERD. It will also sometimes identify the presence of a hiatus hernia and the position and function of the Lower Oesophageal Sphincter which is necessary prior to performing Impedance reflux studies.
- Reflux physiology studies. When GERD is thought to be responsible for dysphaia and anti-reflux surgery is being considered reflux studies are always performed. These are;
- 24 hour catheter reflux monitoring. A small tube (catheter) is inserted through the nose to the bottom of the oesophagus and measures reflux events usually over 24 hours at the bottom as well as the top of the oesophagus. It will also include a pH sensor in the stomach to ensure normal acid production. The catheter is attached to a recorder about the size of a mobile phone and patients can record when they experience symptoms allowing correlation between the two. These are known as “symptom associations”. pH testing assesses acidic/non acidic reflux events. Modern testing includes impedance which offers the advantage that it also distinguishes between liquid, solid and gas reflux events. So, for instance impedance can identify belching and its relationship with reflux.
- Oesophageal pH capsule reflux test. The Bravo test involves attaching a tiny capsule during a gastroscopy onto the lining of the oesophagus just above the stomach. This records acid reflux over a period of 48-96 hours. Instead of a catheter it sends the data wirelessly to a recorder and falls off after the test is complete. The procedure is usually performed under conscious sedation. - CT scanning. Sometimes imaging particularly CT scanning may be employed to assess for structural abnormalities.
What are the treatments for dysphagia?
Reaching the right diagnosis is key to planning treatment. Sometimes simple dietary medication such as eating sloppy foods is all that’s necessary. Some patients will benefit from working with a speech and language therapist and when malignancy is identified this should be treated. Other specific causes of dysphagia are treated in a tailored approach. For instance, Eosinophilic Oesophagitis is treated with topical steroids and/or exclusion diets.
Dysphagia associated with GERD often settles with changes to anti-acid medications and where strictures are identified balloon dilatation (stretching the narrowing during an endoscopy) is indicated. When primary oesophageal motility disorders such as achalasia are diagnosed specific treatment options will be indicated.
In patients considering anti-reflux surgery assessment of oesophageal function is important in all patients. Pre-operative dysphagia can suggest increased risk of post-operative swallowing difficulty. We therefore always recommend high resolution oesophageal manometry to assess motility as this can influence suitability for surgery and the right choice of procedure.